|
Introduction |
Handling Resection Margins |
Click the section headings (in blue) to expand or collapse the content
 Definition of Resection Margin
Definition of Resection Margin
A surgical resection margin is defined as a disrupted tissue plane/surface/edge resulting from artificial (surgical) separation from the rest of organs per procedure. This definition specifies three characteristics of a surgical resection margin of a specimen. A clear remembrance of this characteristic can weed out most potential confusions in the identification and assessment of resection margins.
First, a margin must be a new tissue plane of separation, resulting from a procedure (rarely resulting from trauma tear). For example, an intestinal serosa with tumor deposits that do not adhere to other organ structure is not a margin. Similarly, the right middle lobe of the lung obtained by lobectomy typically has one resection margin, i.e., the hilar margin. However, if the visceral pleura of the lobe has adhered to the chest wall or an adjacent lobe, the area of adhesion has to be dissected surgically and, hence, becomes a margin.
Second, the margin of a resected specimen depends on its relationship to other parts or tissues that remain within the body. For example, if a long segment of small intestine is resected as two or more shorter segments for ischemia infarct in one operation, only one end of the most distal segment and one end of the most proximal segment should be designated as resection margin where the specimens are separated from the rest small intestine still in the body.
Third, a resection margin is a specimen attribute specific to the procedure. For example, a leg stump by above-the-knee amputation following prior below-the-knee amputation only has one (proximal) resection margin (ōper procedureö) since the distal end is the result of a prior surgery.
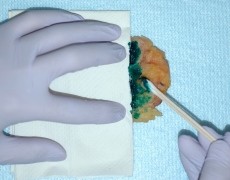
The purpose of specimen inking during gross examination is to accurately and faithfully transmit information to allow accurate and reliable microscopic assessment of the resection margins. Thus, the correct inking 1) should be confined in its margin area, 2) survive subsequent tissue processing and 3) should be clearly and unequivocally visible under the microscope. Unfortunately, this simple procedure is rarely done correctly. The following is recommended inking method:
- Blot-dry specimen with paper towel to get rid of excessive liquid on the surface to be inked.
- Identify margin area to be inked, cover adjacent surface with folded paper towel to prevent contamination
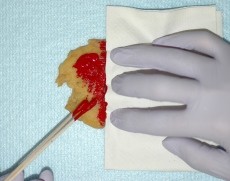
- Use cotton swab soaked with Indian ink to paint the margin area; then let the ink air-dry for up to a minute
- Wet the inked areas with a thin paper soaked with Bouin’s solution (or cover the area with the paper then gently spray Bouin’s solution to the paper).
- Blot-dry the inked surface with a clean paper towel.
It is highly desirable to ink the specimen in a consistent fashion in terms of color in relation to the specimen aspects.ĀSee recommended color schema.
|
|
|
|
|
|


 Other tips to minimize cross-contamination
Other tips to minimize cross-contamination
|
|